Arterial hypertension (hypertension) - syndrome of increasing systolic blood pressure (hereinafter referred to as the garden) ≥140 mm Hg. Art. and/or diastolic blood pressure (hereinafter referred to as DAD) ≥90 mm RT. Art. The primary (essential) and secondary (symptomatic) arterial hypertension is distinguished. The primary prevails among all forms, its prevalence exceeds 90 %. Secondary hypertension is much less common. This type is due to the known reason that can be eliminated using the corresponding intervention. Arterial hypertension, being the main risk factor in the development of myocardial infarction, stroke, chronic kidney disease, causes restructuring of both small and large arteries [1].
Efficacy of Mexidol® therapy for cognitive impairment in patients with arterial hypertension (high blood pressure)

Arterial
hypertension.
Definition
The relevance of the problem
and etiopathogenesis
Increased blood pressure makes a significant contribution to an increase in the disability and mortality of the adult population of developed countries [2]. According to world statistics, the prevalence of hypertension among the adult population is in the range of 30–45 % [3]. The results of a major epidemiological study of ESSU-RF-2 (“Epidemiology of cardiovascular diseases in the regions of the Russian Federation”) showed that from the mid-1990s to 2017 there was an increase in the percentage of men, patients with AG-from 39.2 % to 49, 1 %. At the same time, this indicator in women during the same period decreased from 41.1 % to 39.9 %.
Standardized by age The prevalence of AH in the Russian Federation based on the results of this study was 44.2 %. The increase in the incidence of AH in people not only elderly, but also young age was noted. Among all persons with AH, only 24.9 % carry out regular control of blood pressure, traditionally more often - women, 34.1 %, 16.5 % - men [4]. The interconnection of the level of the garden is proven above 140 mm Hg. Art. With an increase in mortality and incapacity for work due to cardiovascular complications. Thus, it is proved that the growth of the clinical garden above this level is associated with an increase in the risk of stroke, myocardial infarction, cardiac and renal failure [5].
The predisposing
factors of AH development
include: [6-8]
- 1. Age (as age increases, the frequency of AG occurrence increases).
- 2. Improving body weight and obesity.
- 3. Injured heredity (an increase in blood pressure occurs approximately 2 times more often among persons in whom one or both parents had Ag. Epidemiological studies showed that about 30 % of blood pressure variations in various populations are due to genetic factors).
- 4. Excessive consumption of table salt.
- 5. Smoking.
- 6. Abuse of alcohol.
- 7. Hypodynamia.
In the process of increasing blood pressure, the following changes in hemodynamic indicators play the key role:
- increase in general peripheral vascular resistance;
- an increase in cardiac output (minute volume);
- An increase in the volume of circulating blood.
The most important links in the pathogenesis of the primary (essential) hypertension are: activation of the sympathydrenal system (CAS), renin-angienzine-aldosterone system (RAAS), violation of Kationov’s membrane transport (Na+, Ca2+, K+), increase in reabsorption of kidney sodium, dysfunction of endothelia With a predominance of the products of vasoconstrictor substances, structural changes in the vascular wall of the arteries of the muscle (resistive) and elastic type, impaired microcirculation (decrease in capillaries density), violation of the basic receptor system of the central regulation of blood pressure levels and increasing the rigidity of large blood vessels [9].
Symptoms and clinical examination of the patient with AG
Despite the increased blood pressure, patients with AG may not make any complaints at all. The absence of complaints for a long time can be dangerous for the patient, as it does not signal the need to start the treatment of hypertension in a timely manner.
First of all, patients with AH are complaining of headache,
dizziness, deterioration, forgetfulness, general weakness. This is due to
the fact that the first target organ that the AG strike takes on is
the brain. Cerebral symptoms often serve as a reason for the treatment
of patients to the doctor and the beginning of the treatment of hypertension.
As AH progresses, other organs (heart, kidneys, retina, etc.) are involved in the pathological process, which leads to new complaints (on shortness of breath, chest pain, swelling, visual impairment, etc. One of the most significant The clinical manifestations of AG are considered to be a hypertension (Civil Code). Aimed at establishing the causes of AH and determining its stage.
Mandatory in patients with AH, it is necessary to assess the neurological status and cognitive functions (KF) in order to maximize the early detection of vascular cognitive impairment (SKN). It is also important to conduct auscultation of the heart and carotid arteries. Using instrumental methods, it is necessary to assess the condition of the fundus to detect hypertensive retinopathy [10]. Patients with AG in combination with cerebrovascular diseases (CVP) or signs of atherosclerotic lesions of the vessels of the head and neck are recommended by duplex scanning of brachiocephalous arteries to detect atherosclerotic plaques and/or stenosis of internal carotid arteries [11].
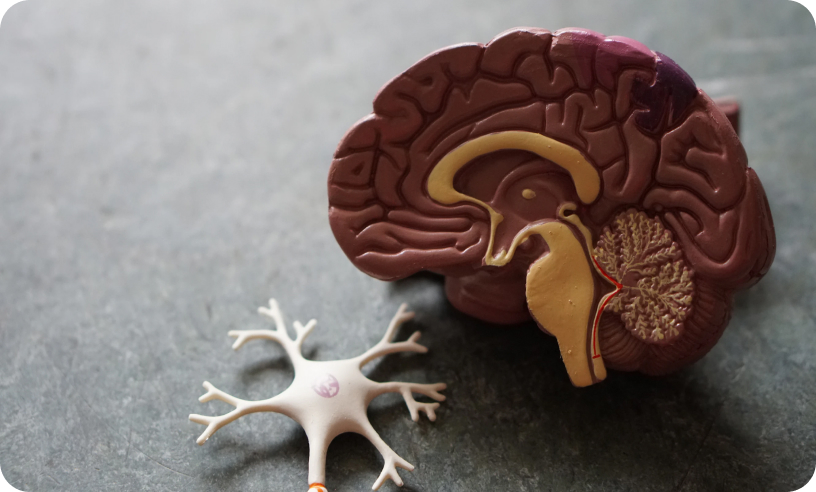
The brain-the target organ of arterial hypertension
The brain is one of the main target organs Ag. The most common cerebral symptoms of hypertension should include headaches mainly in the nape area, as a rule, in the morning, dizziness of varying severity, noise in the ears and visual impairment. With hypertension, extracerebral, intracerebral arteries and microcirculatory channel are affected. Due to the development of hypertrophy of the muscle membrane of the vessels, stenosis and obstruction of the lumen are formed, which leads to brain ischemia:
- acute - ischemic stroke (AI), transient ischemic attack (TIA);
- Chronic - chronic brain ischemia (chemical).
Also, against the background of a long -term existing increase in blood pressure, the development of hemorrhagic cerebral complications is possible - hemorrhagic stroke (GI), subarachnoid hemorrhage (SAK). Hemorrhage can have a secondary character and develops in the zone of ischemic brain damage. The most dangerous complications of AH are cerebral vascular disasters.
Ischemic stroke (AI) occupies one of the first places among the causes of death and persistent disagreement of patients with AG. According to The 2016 Global Burden of Disease, published in 2019, every fourth person will transfer a stroke throughout his life. Every year, the world predicts the development of 9.6 million strokes with an increase in the incidence as the population is aging, while 85 % of cases falls on the share of ischemic stroke [12]. In patients with AH, both large and small vessels suffer. As a result of damage to the small cerebral vessels in hypertension in the pathological process, the white substance of the brain is involved. This pathology is called the "disease of small vessels" (BMS) or cerebral microangiopathy. BMS is detected in almost half of patients with AG [13, 14]. The first symptom of brain damage to arterial hypertension (a manifestation of BMS) is a deterioration in cognitive functions, which largely affects the quality of life of patients [15].
Disorders of cognitive functions against the background of arterial hypertension are manifested primarily by the deterioration of control functions. The abilities to switch from one type of activity to another are violated, a deterioration in planning skills, adaptation to the changing conditions of the environment. The concentration of attention suffers, difficulties in the perception of volumetric images in space arise, and there is a slowdown when performing situational tasks. The relationship between the degree of increase in blood pressure in the middle age and the severity of cognitive dysfunction in these patients when they reach the elderly is proved [16].
Cognitive functions and their value
Cognitive, or cognitive, activity is one of the most important manifestations of the functioning of the brain. Cognitive functions provide a person’s connection with the outside world, determine his personality, allow a person to receive and analyze information, store it in memory, acquire and maintain knowledge and skills throughout life, make conscious decisions, and carry out communication with other people. Cognitive functions include memory, attention, gnosis, praxis, speech, social intelligence and control functions (tab. 1) [13].
Function
Gnosis
Praxis
Speech
Memory
Social intelligence
Attention
Managing functions
Description
Perception, the ability to create holistic images (for example, the ability to recognize people's faces)
The ability to absorb motor skills (for example, the ability to dress, hold a spoon, comb your hair)
Understanding the addressed speech, the ability to express their thoughts in words
The ability to capture, save and play information
The ability to understand and interpret the emotions and behavior of other people
The ability to quickly respond to incentives and maintain the level of activity necessary to perform work
Planning, control, goal -setting
Table 1. Types of cognitive functions and their description
Disorders of cognitive
functions
Cognitive disorders are different in gravity of violations of higher mental functions (attention, memory, gnosis, praxis, speech, thinking, etc.) as a result of diseases of the brain. The classification of cognitive disorder in severity is of greatest importance. Moderate and severe cognitive disorders (dementia) are distinguished. Moderate cognitive disorders are characterized by a decrease in cognitive abilities, which goes beyond the limits of the age, educational norm, which is reflected in the patient's complaints and can be noticeably others.
However, the presence of moderate cognitive disorders does not lead to significant difficulties in everyday life and is not accompanied by a change in social household and professional activity, with the exception of their most complex types. Moderate cognitive disorders are also called dodement. In cases of severe (demented) cognitive disorders, there is a decrease in cognitive abilities, which leads to significant difficulties in everyday life, partial or complete loss of independence and independence [17].
Features of cognitive disorders in patients with arterial hypertension
The cognitive safety of patients depends on their age, determined by genetic factors, control of blood pressure (by finding blood pressure in the target range), cognitive reserve and the presence of concomitant neurodegenerative pathology [18]. The clinical picture of cognitive disorders varies depending on the disease that causes them. For patients with cognitive disorders against the background of arterial hypertension, at an early stage of memory disorder, they are less characteristic.
In patients with arterial hypertension, controller functions (cognitive processes for planning and controlling current activities), the ability to switch from one type of activity to another, the skills of planning everyday life, adaptation under changing environmental conditions are primarily suffered; reduction in concentration; visual-spatial disorders (difficulties of drawing volumetric images); Slow down in the performance of cognitive tasks [13].
The forecast of cognitive disorders
for arterial hypertension
The rate of progression of cognitive disorders depends on the nature and severity of the disease, but in general for five years in 60 % of patients with moderate cognitive disorders that do not receive the necessary treatment, dementia develops.
Due to the presence of the relationship between the degree of increase in blood pressure in the middle age and the severity of cognitive dysfunction in these patients when they reach the elderly, early diagnostics and timely start of effective therapy, as well as constant observation by the doctor.

Adequately selected antihypertensive therapy can reduce the risk of developing moderate cognitive disorders and dementia in patients with arterial hypertension [19]. Good results of such therapy were shown by Mexidol®. Mexidol® with cognitive disorders significantly improves cognitive function in patients with AH with course treatment. In the event that the patient reveals signs of a violation of cognitive functions, then they must necessarily undergo a number of examinations, including neuropsychological testing using valid scales to evaluate cognitive functions [20].
Diagnosis of cognitive
disorders
The main scales that are used to examine the patient with cognitive disorders [16]:
- Montreal scale for assessing cognitive functions (MOCA - produces a screening assessment of the presence of cognitive disorders, and is also used to assess the dynamics of changes in the cognitive status of patients);
- The Mini-Mental State Examination scale (MMSE)-evaluates the severity of cognitive disorders;
- Watch drawing test - a test for determining the severity of cognitive disorders and differential diagnosis of dementia;
- The test for the selection of numbers for characters (DSST) detects the first signs of impaired cognitive functions in the patient.
Thus, the timely diagnosis and correctly selected treatment can reduce the progression of cognitive disorders and improve changed functions.
The possibilities of cerebrotrotation in the treatment of cognitive disorders for arterial hypertension
According to many experts, for most patients with cerebrovascular diseases, including against the background of arterial hypertension, a neuroprotection program is necessary for the prevention and treatment of cognitive disorders. The key role in it is given to drugs of the neuroprotective series. The choice of a neuroprotector should be based on a evidence base confirming not only its effectiveness in the correction of cognitive disorders, but also good tolerance of therapy. The multimodal mechanism of action of the drug is also needed, which allows reducing the amount of drugs taken and thereby eliminating the possibility of polypragmasis, as well as the absence of undesirable interlerable interactions with basic therapy drugs [21]. One of these drugs is the original Mexidol®.

Mexidol® in the treatment of cognitive disorders
Mexidol® is a vivid example of the achievements of the Russian pharmaceutical industry. It is a unique domestic development of scientists of the State Research Institute of Pharmacology of the RAMS [22]. Two related and functionally significant compounds are based on the drug Mexidol®: 2-ethyl-6-methyl-3-hydroxypyridin and succinate. The combination of these components determines the multimodal properties and a wide range of pharmacological effects of the drug. The main pharmacological effects of the drug Mexidol® include antioxidant, antihypoxic and membrane -stabilizing. The antioxidant and antihypoxic effect of Mexidol has been proved in numerous experimental and clinical studies [21]. Thanks to multimodal properties, Mexidol® is provided by nootropic, anti -amnestic, anxiolytic and other effects [23]. The presence in the composition of the succinate stimulates the formation of ATP molecules in mitochondria. Mexidol® with cognitive disorders activates the process of energy formation, prevents the development of intracellular acidosis, which retains the functioning of neurons. Succinate stimulates tissue breathing, in conditions of a lack of oxygen activating the Crebs cycle and thus increases the content of ATP and creatine phosphate. The pyridin base in the molecule of the drug Mexidol® provides neutralization of free radicals and stimulates the cellular protection system from them, also ensures stabilization of cell membranes. All this prevents the damage to cells and their death. Thus, Mexidol®, with cognitive impairment, increases the resistance of cells and tissues to hypoxia and oxidative stress.
Mexidol® is an original drug. It is the first time a synthesized active molecule, which has passed a full cycle of preclinical and clinical studies that proved the effectiveness of the drug. At the moment, there are more than 20 generics of the original Mexidol® preparation. Generic is usually a cheaper copopia, produced by another manufacturer based on the same active substance as the originator, after the expiration of its patent protection. Generic can differ from the original efficiency and safety due to the lack of the results of a randomized clinical test (RCT), differences in the composition of excipients, deviations of pharmacokinetic indicators within ± 20 % [24]. The high safety and effectiveness of the drug Mexidol® are demonstrated in the treatment of cognitive disorders in patients with cerebrovascular diseases such as chronic brain ischemia with concomitant arterial hypertension and without it. Mexidol® for memory and attention also has a favorable effect.

In a multicenteric randomized doubles of a placebo-controlled study of Memo (Mexidol-chronic brain ischemia), 318 patients (age-40–90 years) with chronic brain ischemia took part. Patients were randomly divided into 2 groups. In the main group, patients received prolonged sequential therapy with Mexidol® according to the: Mexidol® dose of 500 mg per day intravenously for 14 days with the subsequent transition to the tablet form of Mexidol® Fort, 1 tablet three times a day on the background of the basic therapy for 60 days. Patients of the control group, together with basic therapy, received a placebo according to a similar scheme. As the primary criterion for effectiveness, the average value of the change in the point on the Moca scale at the stage of completion by the patient completion of the study compared to the initial level was chosen.
By the end of the observation period (75th day), the group with the drug Mexidol® noted and normalization of cognitive functions: +4.22 points on the Mosa scale with a total score of 26.22-the norm (VS 2.17 points in the placebo group, total The score amounted to 24.17 - cognitive disorders), +8 points for the dough of digital characters (VS +5 points in the placebo group). The results indicate the high efficiency of sequential therapy scheme Mexidol® and Mexidol® Fort 250 in the correction of cognitive disorders in patients with chronic brain ischemia [23].
Go to the study of memesAs part of Subanalysis of the study of Memo, patients with
chronic brain ischemia were divided into 4 subgroups:
1. Patients with AG who received consistent therapy with Mexol® according to the scheme: Mexidol® + Mexidol® Fort 250 (n = 144); 2. Patients with arterial hypertension receiving placebo (n = 146); 3. Patients without arterial hypertension who received consistent therapy according to the scheme: Mexidol® + Mexidol® Fort 250 (n = 15); 4. Patients without arterial hypertension receiving placebo (n = 12). At the end of the observation period, statistically significant differences in the dynamics of the Mosa scale between groups of patients receiving Mexidol® and placebo were identified, which indicates the superior effectiveness of therapy with Mexidol® and Mexidol® Forte 250 in the subgroup of patients with AH. Against the background of therapy with Mexidol®, unlike placebo, the median value of the point on the Mosa scale at the end of the observation period reached the level of the norm in all patients. A comparable nature of the safety profile with Mexidol® and placebo is established.
Thus, the results give reason to recommend the long-term consistent use of Mexidol® and Mexidol® Fort 250 in the complex treatment of patients with arterial hypertension and chronic brain ischemia as an effective tool to protect the brain and means of pathogenetically substantiated therapy for cognitive impairment [ 25]. Effective treatment scheme Mexidol® and Mexidol® Fort 250 for cognitive disorders - Mexidol® at a dose of 500 mg per day intravenously for 14 days with the subsequent transition to a tablet form of 250 1 tablet 250 mg three times a day for a day for a day for a day 60 days. Courses at least twice a year.

How to take Mexidol® for hypertension?


Block of articles on this topic
List of literature
24. Original drugs and generics: evidence -based conformity factor // Pharmaceutical Bulletin, No. 38, 2013, p. 12.
THE INFORMATION IS INTENDED FOR HEALTHCARE AND PHARMACEUTICAL PROFESSIONALS. THIS INFORMATION IS NOT INTENDED AS A SUBSTITUTE FOR MEDICAL ADVICE.
Source of photos and images Shutterstock.com